



Patients must undergo a careful diagnostic workup to stage their disease. Before developing active myeloma, patients pass through two earlier disease stages. These precursor stages are monoclonal gammopathy of undetermined significance (MGUS) and smoldering multiple myeloma (SMM).
What Is MGUS?
The earliest stage of myeloma is not cancer at all. Rather, this stage is a benign condition called monoclonal gammopathy of undetermined significance. Shortened as MGUS, it is pronounced "EM-guss."
- MGUS patients have:
- a low level of a type of blood protein (monoclonal protein, also called M-protein)
- a low level of abnormal plasma cells in the bone marrow,
- no indicators of active disease.
- All patients with active myeloma once had MGUS.
- Only 20% of patients with MGUS actually progress to active myeloma.
- The risk of a patient's progression from MGUS to active myeloma is only 1% per year.
- A hematologist/oncologist (a specialist n cancers of the blood) should monitor patients with MGUS.
- MGUS patients do not need to undergo treatment unless they choose to take part in a clinical trial.
What Is Smoldering Multiple Myeloma?
Smoldering multiple myeloma (SMM) is
- asymptomatic
- an intermediate stage of myeloma between MGUS and active myeloma
- Patients with SMM have a higher level of monoclonal protein and more abnormal plasma cells in the bone marrow than patients with MGUS.
- These patients do not have any CRAB criteria (measurement of end-organ damage), or damage to red blood cells, kidneys, or bones.
- SMM can be thought of as a range of different stages of disease with three distinct possibilities:
- MGUS with a higher but stable number of abnormal plasma cells.
- Minimally progressive myeloma without CRAB criteria or myeloma-defining events.
- Moderately progressive myeloma, but with no damage to red blood cells, kidneys, or bones.
Your doctor should monitor your status regularly. Be sure to inform your doctor about any changes in your health status.
- The risk of progression to active myeloma for patients with standard-risk SMM is:
- Ten-percent (10%) per year for the first five years
- Three-percent (3%) per year for the next five years
- One to two-percent (1-2%) per year for the next 10 years.
- The standard of care for SMM is not to treat the patient but to "watch and wait."
- There are clinical trials available to treat patients with SMM and "high-risk" SMM before their disease progresses.
- Consult a hematologist/oncologist to tell apart MGUS, SMM, and active myeloma.
- If possible, consult with a myeloma specialist to avoid either unnecessary or delayed treatment.
What Is Active Myeloma?
- Active myeloma may be diagnosed for either of the following reasons:
- Specific tests show a risk of progression to CRAB criteria within 18 months to 2 years. CRAB criteria include damage to bones, red blood cells, and/or kidneys.
- The patient already has one or more of the CRAB criteria.
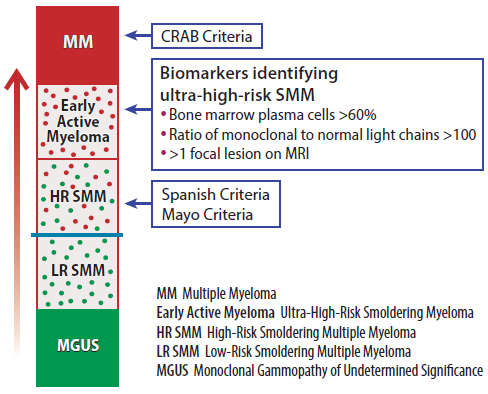
- Until 2014, patients were not diagnosed with myeloma unless they had one or more of the CRAB criteria. In 2014, the IMF's International Myeloma Working Group (IMWG) published new diagnostic criteria based on biological markers. These markers could predict that one or more of the CRAB criteria would occur within 18 months to 2 years in patients with "ultra-high-risk myeloma."
- "Myeloma-defining events" (MDE) are another name for these biological markers.
- "Early active myeloma" is the new definition of "ultra-high risk myeloma." Healthcare professionals recommend treating "early active myeloma."
Definitions of MGUS, SMM, and Myeloma
| NAME | DEFINITION |
| Monoclonal gammopathy of undetermined significance (MGUS) | · Monoclonal protein present but usually ‹ 3.0 g/dL · No CRAB features or other indicators of active myeloma · Bone marrow monoclonal plasma cells ‹ 10% |
| Smoldering multiple myeloma (SMM) |
· Higher level of disease than MGUS: serum M-component can be › 3.0 g/dL and/or bone marrow plasma cells › 10% and < 60% but Both criteria must be met: 1. Serum monoclonal protein (IgG or IgA) ≥3 g/dL, or urinary monoclonal protein ≥500 mg per 24 h and/or clonal bone marrow plasma cells 10 to < 60% 2. Absence of myeloma defining events (MDE) or amyloidosis |
| Myeloma based on MDE | · ≥ 60% bone marrow plasma cells · Free light chain ratio ≥ 100 · > 1 MRI focal lesion |
| Myeloma based on CRAB | · Monoclonal protein present, and · One or more CRAB features and/or indicators of organ damage |
*Organ damage classified as "CRAB" or any other significant clinical problem linked to myeloma progression such as recurrent infections or neuropathy (nerve damage) unrelated to treatment.
C - Calcium elevation (> 11mg/dL).
R - Renal dysfunction (Serum creatinine > 2mg/dL or creatinine clearance (< 40mL/min).
A - Anemia (hemoglobin < 10g/dL or > 2g/dL decrease from patient's normal).
B - Bone disease (≥1osteolytic lesions detected on skeletal radiography, WBLC CT or PET/CT).
One or more "CRAB" features or other significant problem required for diagnosis of symptomatic myeloma.
New Definitions of Myeloma and Early Myeloma
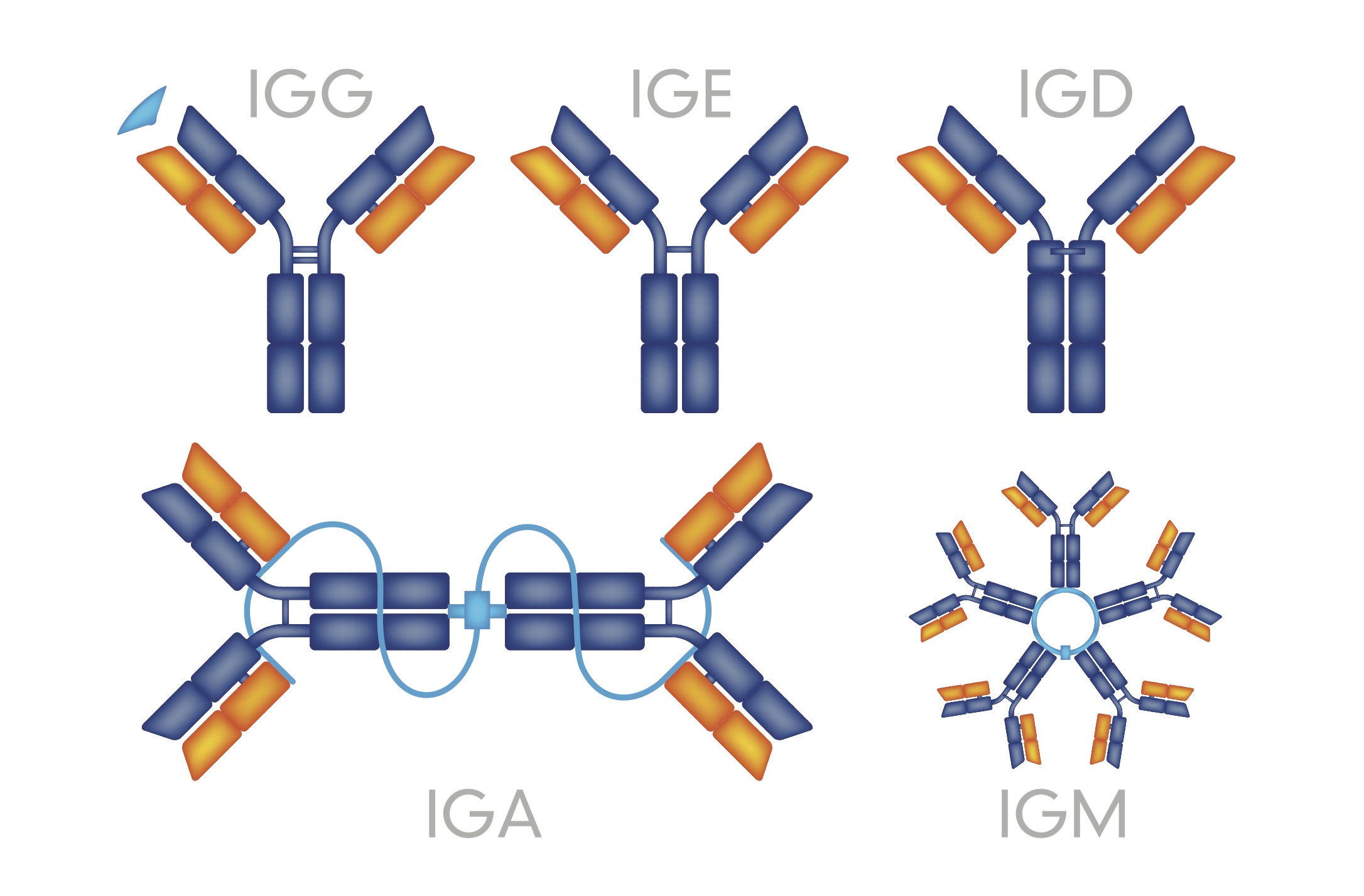
Myeloma is a cancer of the plasma cells. Plasma cells are white blood cells that make antibodies. In medical terms, these antibodies are complex proteins called "immunoglobulins." They fight foreign substances such as bacteria and viruses.
Myeloma cells, unlike healthy plasma cells, cannot make functioning antibodies. Instead, they make an abnormal immunoglobulin known as "monoclonal protein." This results in a reduced ability to fight infection. Myeloma grows within the bone marrow. The presence of immunoglobulins may also cause other problems within the bone marrow and/or outside the bone marrow.
Medical Problems Related to Myeloma
What’s Next?
Understanding the type of myeloma you have will help you and your healthcare team assess how your disease may progress and how it should be treated.
The International Myeloma Foundation medical and editorial content team
Comprised of leading medical researchers, hematologists, oncologists, oncology-certified nurses, medical editors, and medical journalists, our team has extensive knowledge of the multiple myeloma treatment and care landscape. Additionally, Dr. Brian G.M. Durie reviews and approves all medical content on this website.
Last Medical Content Review: June 6, 2021